July 26, 2008
 Krankenkassen and federalism
Krankenkassen and federalism
Obama was a bit uncomfortable in Berlin facing Bismarck's OTT Siegessäule, an eyesore from Schinkel's elegant Brandenburg gate a kilometre to the East where he was speaking
[Update: he was speaking under the Siegessäule. But I'm still right
about the Brandenburg Gate.]. He didn't mention that his universal health insurance plan
is basically a clone (via Edwards and Clinton) of the cunning old
warhorse's revolutionary 1884 law. This also left an existing patchwork
of enterprise-based plans in place, adding a default public one. So
I'll call Obama's scheme by its Bismarckian name: a Krankenkasse.
The Germans are still content with this system. The default public scheme, the Allgemeine Ortskrankenkasse (AOK), was originally based on local government units, not the crazy quilt of kingdoms and duchies that Bismarck had welded into the Second Reich, from Prussia (pop.>25m) to Saxe-Coburg-Gotha (pop.<250,000). Now the AOK has been fitted into the 16 tidy Länder of postwar federal Germany. But it looks to me as if this is just an administrative division, and the AOK is really a centralized national scheme.
Is Obama's plan for a federal or a national Krankenkasse?
His website points both ways (my italics):
(1) Obama will make available a new national health plan which will give individuals the choice to buy affordable health coverage that is similar to the plan available to federal employees. ...One legitimate worry about national welfare programmes in the USA, from the New Deal onwards, is that that they have tilted the constitutional balance further towards Washington and away from the states. So it looks to me desirable to try to minimize this drift by making the krankenkassen as autonomous as possible, with strong ties to the states, and capable of innovation within a clear framework of national standards.
...
(6) ... The Obama plan is a national one that builds on these efforts [by states], and it will not replace what states are doing. Indeed, states can continue to experiment, provided they meet the minimum standards of the national plan.
But if you set up a state-based system, most of the resulting KKs would be too small. What's the size range for an efficient health care provider? The much praised Veterans Administration health care system covers 7.8 million. The NHS in England (50m) has chronic management problems, while the now autonomous Welsh (3m) and Scottish (5m) baby NHSes seem to work better. The successful national systems of the continental Nordic countries have coverages between 5 and 9 million, though those of the Nordic islands are perforce much smaller. I suggest setting 3-5m enrollees as the target range. The lower limit corresponds to Wales, the upper one to Scotland, Denmark and Finland. [Update in footnote.]
Obama'a KKs won't cover everybody or even the majority. The German AOK has 37% of the market, after 124 years. Let's award its American progeny a generous 25% market share. So the desirable catchment population is 12m - 20m. Only six US states meet the Welsh limit: California (37m), Texas, New York, Florida, Illinois, and Pennsylvania (12m.). Only California and Texas meet the Scots one.
Accordingly if you want capable, innovative, independent-minded KKs you have to go for regional groupings. That's how it works for other functions: the original 7 Baby Bells; the 9 FAA regions for air traffic control; and the 12 banks of the Federal Reserve system.
It would be a mistake to define the health regions top-down. Instead Obama's Health Secretary should set a minimum catchment size and invite the states to form groupings to meet it.
[Addition 27/7 The alternative is a giant national system, an American version of the AOK - Allgemeine Obam'sche Krankenkasse. This would cover 76 million Americans on the same projection, one-and-a half times the size of the English NHS. How could such a mighty behemoth avoid becoming remote, unresponsive, and unmanageable?]
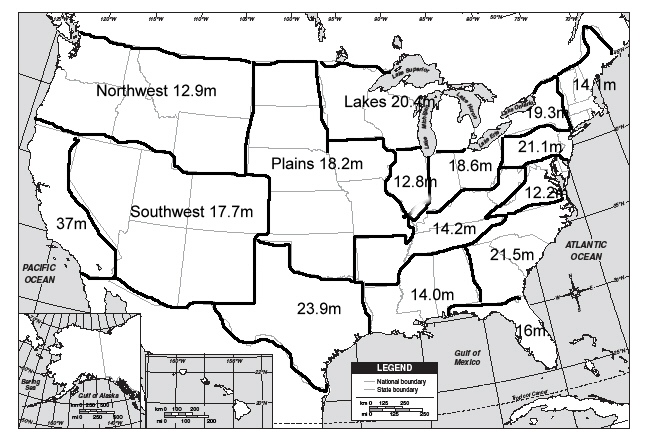
Here's a map I've doodled using the 12 million cutoff. It gives 15 regions for the continental United States, with I fancy a quite high level of cultural affinity. Alaska and the Pacific islands would have their own smaller regions, since the distances make anything else artificial. NB This is not a proposal, but it shows my idea is geographically feasible. [Update Population data by state here or here. Outline map to play with here.]
C.T, a friend who consults internationally on health care reform writes:
Definitely think you are right about the optimal size in terms of organisation of health care financing. I have long thought that the success of social protection in the Scandinavian countries was largely a function of conveniently sized administrative units and a high degree of cohesion and therefore social solidarity amongst these comparatively small population groups.
Update 2 27/7 - Scandinavia
Jacob Christensen, a Nordic political scientist blogger, comments with useful details on the Scandinavian tax-financed systems.
In Denmark and Sweden, there is no national health care in the strict meaning - regional councils are responsible for running primary and secondary health care. Norway is different these days and there are definitively tendencies towards centralisation of the provision of health care. ...The rule of thumb in Denmark and Sweden seems to be that a health care authority should cover 1-2 million people.These authorities are cradle-to-grave comprehensive service providers, not krankenkassen, operating in homogeneous and egalitarian societies. The Nordic countries have excellent health care systems that deserve careful study, as does the Dutch regulated insurance model. But the priority for Obama, who has made his choice of basic model, must be to learn from the countries that operate something close to it: Austria, Switzerland and Germany.
France has its caisses d'assurance maladie, some territorial and others professional, but SFIK they are all public. Employers often buy their employees complementary private medical insurance, which covers excess fees, single-room hospital charges, and more dentistry and prosthetics. There's no network of employer-based comprehensive caisses in the private sector, so France is not that close to the Obama plan. But the fact that Jacobin France still decentralizes delivery of medical care does reinforce my argument. There is no Médécine Nationale on the analogy with l'Education Nationale. Guess which public service works better.
|
Thread: Europe , Thread: Health Care , Thread: The Obama Presidency



{kind=link}